There is no cure for MVID, and the current treatment options are risky and can limit the patient’s quality of life. Children with MVID should be under the management of specialized pediatric gastrointestinal centers and professionals.
Intravenous nutrition
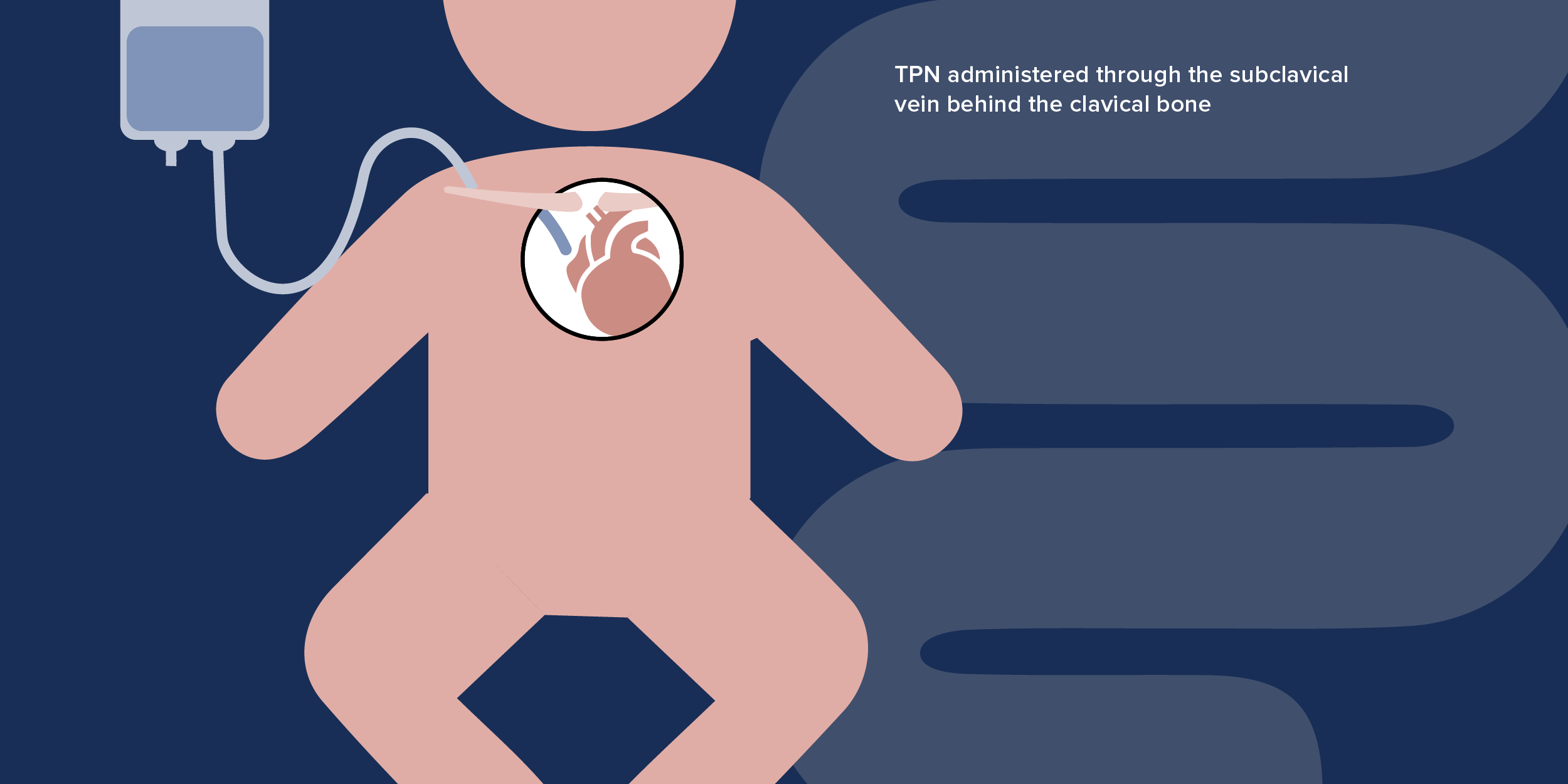
The most common method for managing MVID is parenteral nutrition or PN, in which fluids and nutrients are delivered directly to the bloodstream of the patient, bypassing the intestine. If patients only get nutrition from PN, and nothing is taken by mouth, the procedure is known as total parenteral nutrition or TPN. Because of the persistent nature of the diarrhea, patients often need continuous TPN, up to 24 hours a day.